Truncus Arteriosus
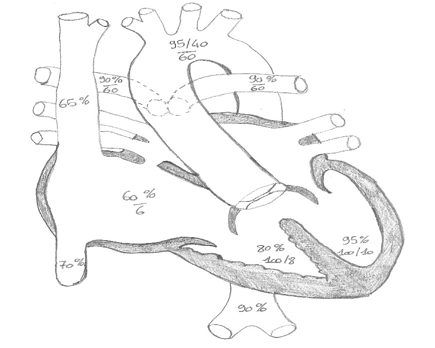
Definition: single arterial trunk and overriding VSD, arising from normally formed ventricles. Absent or diminutive PDA. 100% mortality within the first year if untreated.
Prevalence 3% in CHD.
Incidence 5-15:100.000.
Physiology:
Parallel circulation.
With decreasing PVR there is increased PBF and increased flow to LA and LV, leading to CCF.
Diagnosis:
Presents usually 1-2 weeks postnatally (decreasing PVR) and subsequently CCF with failure to thrive, dyspnea, diaphoresis.
Diagnosis is by echo and in selected cases, cardiac catheterisation.
Preoperative management:
- Balanced circulation (aim for SpO2 75-85%).
- Hypoventilation to increase the PVR and to reduce the SVR. SNP (0.5-4 mcg/kg/min) to lower SVR.
- Aim for a MAP >35 mmHg in neonates.
- Intubate and sedate to lower oxygen consumption.
Preoperative preparation:
ECG, CXR, CUS, FBE, clotting, UECs, FISH, PRBC (4), FFP (2), platelets (2), cryoprecipitate (2).
Methylprednisolone 10mg/kg 12hrs and 6hrs pre surgery in neonates.
Surgery:
Detaching of the PAs, ventriculotomy to close the VSD, valved RV-PA conduit.
In severe truncal valve insufficiency there may be aortic homograft with reimplantation of the coronary arteries.
Postoperative management:
- Keep intubated, ventilated, sedated and paralysed for 24 hours
- Inotropes: milrinone plus dopamine or norepinephrine, aim for MAP >40mmHg in neonates
- Haemodynamics: age adjusted in neonates: SBP >60 mmHg, MAP >40 mmHg (increasing over time), LAP 8-12 mmHg, CVP 8-12 mmHg
- Respiratory: normoxaemia, normocapnea
- Fluid restriction: 1 ml/kg/hr, trophic feeds
- Haemostasis
- Keep normothermic
Specific problems:
- Low cardiac output state: expect 6-12 hrs post bypass
- Pulmonary hypertension crisis: especially in neonates
- Arrthymias: JET – decrease inotropes, overdrive pacing, add noradrenaline, cooling, amiodarone
- Diastolic RV dysfunction: restrictive physiology, usually transient phenomena lasting 48-72 hrs
- Residual truncal valve insufficiency: mild to moderate is usually well tolerated, however if severe may need reinvestigation
Outcome:
Perioperative mortality: 10%
Long term survival after 5, 10, 15 years: 90%, 85%, 83%
References:
[1] Critical Heart Disease in Infants and Children; 2nd ed, Nichols et al: Peristent Truncus arteriosus
[2] Surg Clin North Am. 1949 Aug;29(4):1245-70: Collett et al: Persistent truncus arteriosus; a classification according to anatomic types
[3] Am J Cardiol. 1965 Sep;16(3):406-25: Van Praagh et al: The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its embryologic implications. A study of 57 necropsy cases
[4] Cardiol Young. 2005 Feb;15 Suppl 1:125-31: Backer et al: Techniques for repairing the aortic and truncal valves
All Marc’s PICU cardiology FOAM can be found on PICU Doctor and can be downloaded as a handy app for free on iPhone or Android. A list of contributors can be seen here.


