Transposition of Great Arteries
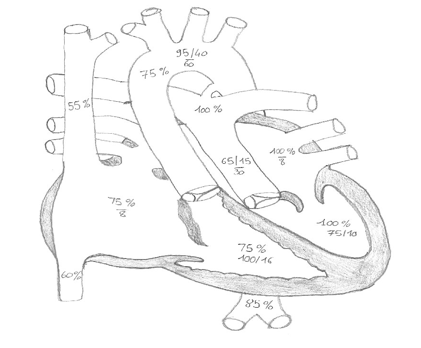
Definition: aorta arising from the anatomic RV, and the pulmonary artery arising from the anatomic LV. Most common form: AV concordance and VA discordance with associated VSD (40%). Coarctation/IAA (10%), LVOTO (10%), coronary branching anomalies (>30%, Leiden classification).
Less common forms: Taussig-Bing anomaly (TGA with outlet VSD & DORV); congenitally corrected TGA (ccTGA, VA discordance and AV discordance).
Physiology:
Amount of mixing is crucial.
TGA/VSD are cyanotic and more prone to CHF, TGA/IVS deep cyanosis and postnatal CVS collapse.
While the RV is abnormally thick walled, the LV is usually thin, and pLV determines the timing of surgery.
Diagnosis:
ECHO.
Postductal SpO2 may be higher than preductal SpO2.
Preoperative management:
Ideal Monitoring: ECG, pre- and post-ductal SpO2, blood pressure, near infrared spectroscopy.
Ideal lines: leave UVC and UAC if surgery within 24-48 hrs; patients on PGE1 require 2x IV access at all times. Consider PICC line if on PGE1 for >48 hrs.
Investigations: echo immediately upon admission, then as per need, or once per week. Echo will attempt to define coronary artery anatomy.
One cranial ultrasound between balloon atrial septostomy and surgery, more as per clinical indication.
Probable therapeutic interventions:
Prostaglandin E1 (PGE1, alprostadil) 200mcg/kg in 50 ml dextrose 5% at 10-100 ng/kg/min.
Balloon atrial septostomy. Indications: if SaO2 <70% on PGE1 (performed via umbilical or femoral vein under echo or fluoroscopic control). Requires anaesthesia, IPPV, and close non-invasive monitoring.
Most children do not need intra-arterial monitoring or insertion of a central line for inotropic administration.
Usual post-procedure plan: wake, wean & extubate, and attempt wean off PGE1 ASAP.
Suggested fluids/nutrition – oral or NG feeds.
Preoperative preparation:
ECG, CXR, CUS, FBE, clotting, FISH, IECs, PRBC (4, irradiated), FFP (2), platelets (2), cryoprecipitate (2).
Methylprednisolone 10mg/kg 12 hrs and 6 hrs pre surgery in neonates.
Surgery:
Timing: depends on pLV and defect (TGA/IVS :10 days, TGA/VSD: 3 mths, Taussig-Bing: 9 mths).
Technique: arterial switch operation (ASO), pulmonary artery banding and systemic shunt in unprepared LV. Mustard/Senning for atrial switch, Rastelli operation for patients with malalignment of VSD and/or LVOTO. Note: ASO possible after Mustard/Senning; may need pulmonary artery banding to retrain LV function.
Monitoring: invasive systemic BP, CVP or RAP, LAP, NIRS, transcutaneous SaO2, inline SvO2, urine output, core temperature.
Lines: right radial arterial line, 3-lumen central line in right IJV, or 2-lumen central line right IJV plus direct RA line, direct left atrial line, 2x peripheral IV access, IDC, advance naso-pharyngeal to -esophageal temperature probe, naso-gastric tube, double atrial and ventricular pacing wires.
Proposed investigations:
- On admission: CXR, ABG and VBG, ACT (and TEG), clotting, FBC, RFT, LFT, electrolytes, BNP, troponin I, 12-lead ECG
- Transthoracic echo as per discussion at handover (LVsystF, LVdiastF, RVF, PAP, PS, AI, coronary blood flow)
- ABG 1-2hrly for the first 6-12 hrs, more frequently in periods of instability or manipulation of inotropes
- Subsequent daily checks: CXR, echo, ABG, clotting, FBC, RFT, LFT, electrolytes, BNP, Troponin I, 12-lead ECG
Probable therapeutic interventions:
- Airway and ventilation: aim for TV 6-8 ml/kg and pCO2 35-40 mmHg, PEEP min 5 cm H2O. If stable at 2 hrs after PICU admission: ET suctioning and standard lung recruitment manoeuvre (PEEP no greater than 15 cmH2O for 2mins, decrements by 5cmH2O every 30secs to 5 cmH2O), which should be repeated after each airway disconnection.
- Antibiotic prophylaxis.
- Prophylactic triiodothyronine.
- Analgesia and sedation: morphine infusion (up to 50 mcg/kg/min), midazolam infusion (maximum 30 mcg/kg/min), IV paracetamol from admission on; if required add dexmedetomidine (0.2-0.7 mcg/kg/min) after cessation of paralysis.
- Paralysis: cisatracurium IV bolus (0.15 mg/kg), then continuously (1-10 mcg/kg/min) until next morning after echo.
- Bleeding from wound or chest drains should be closely observed at all times from time of admission on; output of >10ml/kg anytime, >5ml/kg/hr in the first 2 hrs, or >1ml/kg/hr beyond 4 hrs post-op should result in readiness for administration of blood products, coagulation tests (platelets, INR, APTT, fibrinogen and TEG), and notification of the cardiac surgical fellow. Beware of sudden increase in output as well as a sudden stop!
Cardiovascular agents:
- Dopamine 5-10 mcg/kg/min plus milrinone 0.25-0.75 mcg/kg/min preferably via separate lines; or adrenaline max 0.03-0.08 mcg/kg/min plus milrinone 0.25 0.75 mcg/kg/min via direct RA line if available (adrenaline can go with dopamine line, but preferably not with milrinone).
- Substitution of, or switching off, inotropes should not be undertaken in the first 6-12 hrs post-op.
- Accepted vasodilators in acute phase: milrinone if renal failure (max 0.3 mcg/kg/min) and dexmedetomidine
- Do not cease inotropic support until after extubation (except in longterm MV patients)
Aim for haemodynamic steady-state:
- Defined as SBP >65 mmHg, MAP ≥45 mmHg, LAP 5-8 mmHg, SvO2 ≥60%, lactate <3 mmol/L.
- If intotropic score exceeds 15 (dopamine dose + [100] x adrenaline dose + [10] x milrinone dose in mcg/kg/min): vigorous investigation of causes, and consider reopening of sternum.
- If inotropic score exceeds 20, causes need to vigorously be investigated and/or elective ECLS (VAD or VA ECMO) considered.
- The pacemaker should be readily available, and the sensitivity and output thresholds of pacing wires measured/tested and recorded (pacing).
- Vigorous temperature control (36.5 ± 0.5) from admission is of crucial importance.
- Peritoneal dialysis should be started with low threshold; begin with Physioneal 1.37%, 10ml/kg cycle volumes at room temperature, 1 hrly cycle times, and no additives (heparin or KCl).
Suggested fluids/nutrition/electrolytes:
- Fluid restriction of 30% first 24hrs; as of day 2 50% until extubated; increments of 20ml/kg per day thereafter (max TF (=100%) for IV is 120 ml/kg/day, and for enteral 150 ml/kg/day).
- For maintenance use Hartmann’s & 5% dextrose.
- Start NG feeds at 1 ml/hr (EBM or substitute) 6 hrs post-CPB.
- Vigorous fluid restriction, avoid fluid boluses.
- Keep Mg++>1 mmol/l, K+ 4-5 mmol/l, and Ca++ >1.2 mmol/L at all times (but avoid fast boluses).
Specific problems:
- Low CO 6-12 hrs post CPB: keep paralysed, don’t wean inotropes <24 hours → adaption of the LV for systemic circulation (LCOS).
- Anatomical coronary problems: higher risk if single coronary, or intramural course, or coronary looping (LAD and/or Cx off RCA and vice-versa). May cause ischaemic ECG changes, or ventricular ectopics or arrhythmias. (check ECG, troponin). Conduct early investigations (ECHO, Cathlab).
- Arrhythmia: SVT, JET, AV Block (exclude coronary abnormality).
- Low urine output: start PD.
- Pulmonary artery hypertension (rare) (see pulmonary hypertension)
Expected schedule:
Cease paralysis within 24 hrs; start wake and wean day 2; remove intracardiac lines, chest drains, PD and pacing wires day 2 or 3; extubation expected day 3 (48hrs post-op); discharge to ward day 4; discharge home day 14.
Surgical mortality TGA/IVS <2 %, TGA/VSD <4 %, Taussig Bing 6 %.
Proposed pre-discharge preparations:
- If required, low flow nasal-prong oxygen
- Inotropes ceased
- Increasing enteral, and decreasing iv fluids/feeds
- FBC, electrolytes, RFT, LFT, coag, BNP, troponin I
- 12 lead ECG and CXR and ECHO not older than 24 hrs
- Usual medications with frusemide 1mg/kg 8 hrly and spironolactone 1mg/kg BD, additional afterload reduction with lisinopril 0.1mg/kg daily as per discussion with cardiologist and cardiac surgeons
References:
[1] J Thorac Cardiovasc Surg, 1981 Oct;82(4):629-31: Lecompte at al: Anatomic correction of transposition of the great arteries.
[2] Surgery. 1959 Jun;45(6):966-80: Senning: Surgical correction of transposition of the great vessels
[3] Surgery. 1966 Feb;59(2):334-6: Senning: Surgical correction of transposition of the great vessels
[4] Circulation, 2003;107;996-1002: Hoffmann et al: Efficacy and Safety of Milrinone in Preventing Low Cardiac Output Syndrome in Infants and Children After Corrective Surgery for Congenital Heart Disease
[5] Pediatr Crit Care Med. 2010 Mar;11(2):234-8: Gaies et al: Vasoactive-inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass
[6] Am J Cardiol. 2013 Feb 19. Junge et al: Comparison of Late Results of Arterial Switch Versus Atrial Switch (Mustard Procedure) Operation for Transposition of the Great Arteries
All Marc’s PICU cardiology FOAM can be found on PICU Doctor and can be downloaded as a handy app for free on iPhone or Android. A list of contributors can be seen here.


